Medications to Ease Alcohol Withdrawal
Alcohol withdrawal is not just uncomfortable; for people with significant physical dependence, it can be dangerous. When the body has adapted to regular heavy drinking and alcohol is suddenly removed, the nervous system becomes overexcited, producing symptoms that range from anxiety, tremors, and insomnia to seizures and delirium tremens, a medical emergency. Alcohol withdrawal medications are used during withdrawal to calm that overactivity, prevent the most serious complications, and keep a person safe and as comfortable as possible while the body readjusts.
This article explains the medications commonly used in alcohol withdrawal and what each one does. It is educational, not a treatment plan or a guide to self-detox. Alcohol withdrawal should be managed under medical supervision, because the right medication, dose, and setting depend entirely on the individual. If you or someone you love is considering stopping drinking after heavy use, talk to a medical professional or a medical detox program first.
Why Alcohol Withdrawal Medications Are Used During Detox
Alcohol is a central nervous system depressant. With prolonged heavy use, the brain compensates by ramping up its excitatory activity to stay balanced. Remove the alcohol and that compensation is suddenly unopposed, leaving the nervous system in a hyperexcited state. That rebound is what drives withdrawal symptoms, and in severe cases it is what causes withdrawal seizures and delirium tremens.
Most withdrawal medications work by gently restoring that balance, either by acting on the same calming pathways alcohol affected or by targeting specific symptoms. The clinical goals are straightforward: prevent seizures and delirium, ease the physical and psychological distress of withdrawal, and stabilize the person so they can move into ongoing treatment. Which medications are used, and how, is guided by withdrawal severity, scored with tools such as the CIWA-Ar scale, and by each person’s medical history.
Benzodiazepines: the first-line treatment
Benzodiazepines are the standard first-line medication for moderate to severe alcohol withdrawal. They are the best-supported option for reducing the risk of withdrawal seizures and delirium tremens, which is why addiction medicine guidelines recommend them as the foundation of withdrawal management. They calm the same nervous-system pathways that alcohol acted on, easing the rebound overexcitement in a controlled, taperable way.
Several benzodiazepines are used, and the choice is individualized:
- Longer-acting agents such as chlordiazepoxide and diazepam produce a smooth, self-tapering effect that many clinicians prefer for otherwise healthy patients.
- Shorter-acting agents such as lorazepam and oxazepam are often chosen for older adults or people with liver impairment, because they are processed differently and are less likely to accumulate.
Just as important as the drug is how it is given. In symptom-triggered dosing, a patient is scored frequently and medicated based on the severity of their symptoms, rather than on a fixed clock. Decades of research show this approach tends to use less total medication and shorten the length of detox compared with rigid fixed schedules, while keeping outcomes at least as safe. This is one of the clearest reasons an individualized detox plan is safer than a one-size-fits-all protocol.
One key point: benzodiazepines are used for the short, defined window of withdrawal and then tapered off. They are not intended for ongoing use after detox, both because withdrawal resolves and because benzodiazepines carry their own dependence risk.
Anticonvulsant alternatives: gabapentin and carbamazepine
For milder withdrawal, or when benzodiazepines are not a good fit, anticonvulsant medications such as gabapentin and carbamazepine are recognized alternatives. They can ease symptoms with less sedation and carry less potential for misuse than benzodiazepines, which makes them useful in certain outpatient or lower-acuity situations.
The trade-off is that, for moderate to severe withdrawal, these medications are not considered first-line, because they have not been shown as clearly as benzodiazepines to reduce the risk of seizures and delirium. A clinician weighs all of this, the severity, the person’s history, and the setting, when deciding whether an anticonvulsant is appropriate on its own or whether a benzodiazepine-based plan is safer.
Phenobarbital for severe or complicated withdrawal
Phenobarbital, a barbiturate, is sometimes used for severe withdrawal or when symptoms do not respond well to benzodiazepines. It is powerful and effective in the right hands, but it has a narrower margin for error, so it is reserved for monitored settings and clinicians experienced in its use. It is a clear example of why withdrawal medication belongs in a supervised environment rather than at home.
Thiamine and nutritional support
Thiamine (vitamin B1) is given routinely during alcohol detox, but it is worth understanding what it does and does not do. Thiamine does not directly treat withdrawal symptoms or prevent seizures. Instead, it prevents a separate and serious problem: Wernicke’s encephalopathy, a neurological emergency caused by thiamine deficiency that is common in people with heavy alcohol use and poor nutrition.
Because of this, thiamine is a standard part of care, and clinicians give it before any glucose-containing fluids, since giving sugar first can trigger the very deficiency they are trying to prevent. Folate and other vitamins are often provided alongside it as part of nutritional support, since chronic drinking frequently depletes the body’s reserves.
Adjunct medications for specific symptoms
Some medications are added to a benzodiazepine-based plan to manage particular symptoms, but they are not used on their own to manage withdrawal:
- Clonidine and beta-blockers can reduce the racing heart, high blood pressure, and tremor that come with withdrawal. Importantly, they do not prevent seizures or delirium, and because they can mask the signs clinicians rely on to gauge severity, they are used only as supportive add-ons under monitoring.
- Antipsychotics such as haloperidol may be used for severe agitation or hallucinations, particularly in delirium tremens, but always alongside a benzodiazepine rather than instead of one.
The takeaway is that these are targeted tools for specific symptoms, layered onto the core treatment, not substitutes for it.
What about naltrexone, acamprosate, and disulfiram?
These three medications come up often in conversations about alcohol, so it is worth being clear: they are not withdrawal medications. Naltrexone, acamprosate, and disulfiram are used to treat alcohol use disorder over the longer term, helping reduce cravings or support continued sobriety after detox is complete. They have no role in managing the acute withdrawal period itself.
That distinction matters because it reflects a larger truth about recovery: getting through withdrawal safely is the beginning, not the end. Detox stabilizes the body, but lasting recovery depends on what comes next, which is where these medications and ongoing treatment come in. You can read more about that handoff in why detox is the first step.
Why these medications require medical supervision
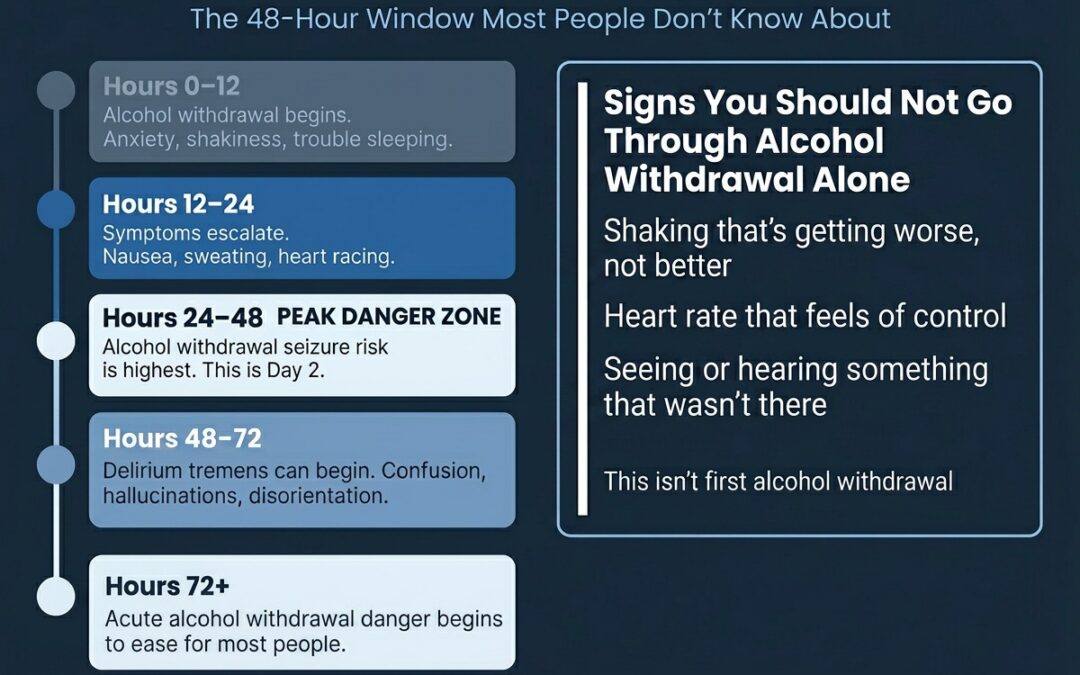
It can be tempting to think of alcohol withdrawal as something to push through alone, but the medications above exist precisely because withdrawal can be life-threatening. Trying to self-medicate, or attempting to taper alcohol without help, is risky: dosing has to be matched to severity and adjusted as symptoms change, withdrawal seizures can appear within hours of the last drink, and delirium tremens can develop a day or two in. Combining alcohol with benzodiazepines on your own is especially dangerous.
In a supervised setting, a care team can assess risk, choose the right medication, monitor vital signs and symptoms, and adjust the plan in real time, including the kind of supportive, stabilizing environment that helps people get through the hardest hours. You can read more about the role of a supportive environment during detox. That oversight is the difference between managing withdrawal safely and gambling with a medical emergency.
Key takeaways
| Medication | Role in alcohol withdrawal |
|---|---|
| Benzodiazepines | First-line; reduce seizures and delirium; tapered off after withdrawal |
| Gabapentin / carbamazepine | Alternatives for milder withdrawal or when benzodiazepines aren’t suitable |
| Phenobarbital | Severe or treatment-resistant withdrawal, in monitored settings only |
| Thiamine (vitamin B1) | Prevents Wernicke’s encephalopathy; not a treatment for withdrawal itself |
| Clonidine / beta-blockers | Adjuncts for heart rate, blood pressure, tremor; do not prevent seizures |
| Naltrexone / acamprosate / disulfiram | Long-term treatment of alcohol use disorder after detox, not for withdrawal |
Get medically supervised alcohol detox in New Hampshire
Liberty Health Services provides medically supervised alcohol detox in New Hampshire, with around-the-clock nursing, evidence-based medication management, and care plans built around each person’s history and needs. If you are thinking about stopping drinking, you do not have to face withdrawal alone or guess at what is safe. Contact Liberty Health Services to talk with a clinical team member about a medically supervised detox program and what to expect.
FAQ
What is the best medication for alcohol withdrawal?
There is no single best medication for everyone. Benzodiazepines are the first-line treatment for moderate to severe withdrawal because they most reliably reduce the risk of seizures and delirium, but the specific drug, dose, and approach depend on the person’s withdrawal severity, medical history, and treatment setting. That is why withdrawal is managed by a clinician rather than self-treated.
Can you detox from alcohol without medication?
People with mild dependence and low risk may sometimes be managed with supportive care, but anyone with moderate to severe alcohol dependence, a history of withdrawal seizures, or co-occurring medical conditions should not attempt withdrawal without medical support. Alcohol withdrawal can become life-threatening, and a medical assessment is the only safe way to know which category you are in.
How long are withdrawal medications needed?
Withdrawal medications are typically used for the acute withdrawal window, often several days to a couple of weeks, and then tapered off. Medications for ongoing alcohol use disorder, such as naltrexone or acamprosate, are different and may be used longer term as part of continuing treatment after detox.
Is it safe to detox from alcohol at home?
For anyone with significant alcohol dependence, detoxing at home without medical supervision carries serious risks, including seizures and delirium tremens. A medically supervised program can provide the right medication, monitoring, and rapid response if complications arise, which is not possible at home.
Related reading
- What Is an Individualized Detox Plan for Addiction?
- Starting Your Recovery: Why Detox Is the First Step
- The Importance of a Supportive Environment During Detox
- Thinking About Getting Sober: Things to Know